In Part 3 of Paying for Primary Care, Gayle Brekke discourses on the behavioral economics of shared health cost arrangements to conclude that insuring primary care adds costs not seen in direct pay. These cost, she contends, simply add on to the 50% administrative cost burden of insurance she had already she had already declared in her Parts 1 and 2. Even though these prior parts featured large overestimates of the burden addressed, at least her assessments in those two parts pointed in the correct direction. In Part 3, Brekke changes heading to go in the wrong direction.
Brekke correctly notes that paying for one’s own health care, and only for one’s own health care, will (almost entirely) avoid a cost pooling process in which payers are at risk of a net transfer of wealth to those who receive more of the covered care than themselves. Because health insurance member payments are pooled and priced in a way that does not directly reflect the varying needs and preferences for receiving health care services, health insurance is one example of a pooling process that is potentially vulnerable to both adverse selection and moral hazard.
A second such vulnerable pooling process is subscription based direct primary care in which unlimited care is promised at a single fixed price that does not directly reflect individually varying needs and preferences.
Here, I discuss why, in today’s healthcare world, subscription based direct primary care is significantly more vulnerable to the difficulties of adverse selection and moral hazard than ordinary health insurance.
Remarkably, advocate Brekke does not admit to the possibility that the problems of behavioral economics that concern her can arise under direct primary care. But arise they will — as actuary Brekke should realize. Nor does advocate Brekke’s analysis take into account the ways in which the health insurance world currently mitigates the same set of problems, e.g., by combining guaranteed-issue, community rating, and risk adjustment under the Affordable Care Act — things we would expect actuary Brekke to address.
Neither adverse selection nor moral hazard (induced utilization) have been incurably problematic in employer sponsored health insurance (ESI). As to the latter, an employer sponsor simply determines the level of employee health care utilization for which he is willing to pay; he can address moral hazard/induced utilization, in its various forms and to the extent he deems appropriate, by adjusting employee deductibles or copayments, and even more complex arrangements like HRAs and HSAs.
As for adverse selection, ESI typically does not offer much in the way of employee choice between plans. Because an employer is generally not allowed to discriminate on the basis of employee health status, when there is employee choice the same plans are available to all employees. When choice is offered, even as the richer plans attract the sicker employees and cost the employer more, the leaner plans will attract the healthier employees and cost less. The costs and savings stay in the corporate family, as it were, and the differences do not by themselves generate net cost increases.
If, as sometimes happens, cross-subsidization between employees picking different plans becomes of concern, employers can get help from qualified actuaries in rectifying the relative pricing of the plans. An elegant extension of such “risk adjustment”, which illustrates in passing how less complex risk adjustment works, can be found here.
As it happens, adverse selection once had overwhelming salience in the market for individual insurance. But things have changed.
A sicker than expected person “adversely selecting” into a benefit rich plan certainly causes that plan’s outlays to be higher than otherwise expected, and some care costs are thereby shifted to other plan members. A shift of the costs of care, however much it may be unhappy financial news for healthier plan mates, does not by itself increase the costs of care. The wasteful, destabilizing aspect of adverse selection is that of having a health care system in which profit-requiring guarantors of the financial costs of health care costs are in a price competition and are, therefore, incentivized to recruit the healthy and reject the sick.
To survive such a competition, particularly in the individual market, insurance companies have historically engaged in risk selection (cherry-picking), incurring heavy administrative costs for underwriting and the like. If companies declined to compete for the best risks, their member pools become smaller and sicker through “death spiral” cycles of healthy member withdrawal and increasing premiums. When companies collectively compete, administrative costs grew from the weight of defensive measures. The end point of all this was the near extinction of the market for individual insurance by the first decade of this century.
Even when adverse election still loomed large, it seems unlikely that the generosity or nuances of plan coverage of primary care had much influence on the decisions of putative adverse selectors. It is the needs and decisions of the sickest patients that matter most to the financial health and stability of insurance plans. Patients so sick that they are comparing plans on the basis of their mOOPs care little about the details of the road on which they will be blowing past their deductible.
Conservatives, provided us with an object lesson, not long ago. The 104th Congress was Republicans first chance in many decades to do something about their dream to privatizie Medicare,. But making that happen is more likely when individual insurance markets are reasonably stable. To stabilize the existing situation in private health insurance, Republicans to implement a major countermeasure against adverse selection in the private-insurance-linked Medicare Advantage program. The innovation allowed the adjustment of the rates paid insurers to fairly reflect the relative health risk of the persons enrolled in their particular plans. In effect, “risk adjustment” required that insurers with low risk member panels subsidize insurers with high risk member panels. This vastly reduced the incentive to cherry-pick and, thereby, carrier vulnerability to adverse selection. Because risk-adjustment mechanisms stabilize private insurance markets they have had support across the Republican spectrum from the Heritage Foundation through Mitt Romney as well as from Democrats.
As under Medicare Advantage and RomneyCare, health insurance policies under the Affordable Care Act have guaranteed issue and are community rated. Underwriting and other practices that discriminate on the basis of health status are barred. And, the ACA extended risk adjustment of insurer payments to the entirety of the individual and small group insurance markets. It is likely the least controversial aspect of the ACA. As noted in multiple actuarial publications, ACA risk adjustment has worked effectively to significantly mitigate the problem of adverse selection. And, even the Trump Adminstration recently bragged about just how stable the individual insurance market has become.
Once the destroyer of the individual insurance marketplace, adverse selection is no longer an overwhelming driver of wasteful overhead costs in the individual insurance market. While risk-adjustment is still being refined, a major part of the work is done.
On the other hand, there is no risk adjustment apparatus to relieve the problem of adverse selection between competing direct primary care subscription plans. There is a substantial incentive for a DPC firm to seek a pricing advantage in order to grow market share; and it can do this by beating its competitors at enrolling lower risk, lower utilization members. A subscription-based D-PCP unwilling to pick cherries can easily be left with a panel of lemons. We know where enrollment races can lead.
A tacit understanding among D-PCPs to refrain from price competition could mitigate the problem, if it held. But competition for direct pay subscriptions is a growing reality; at least one DPC thought leader has already complained of some direct pay price competitors as hijackers, and he promised “push back”, equating them to a venereal disease that needs to be eradicated. I have no doubt that this summer’s Direct Primary Care Summit will have at least one speaker complaining of a “cream-skimming” competitor.
Thanks to legally mandated risk adjustment, the chance of a purchaser of individual health insurance having to bear significant, unnecessary administrative costs resulting from the phenomenon of adverse selection is small, and shrinking. On the other hand, if that phenomenon has real salience for the question of how to pay for primary care, it is because the absence of risk adjustment renders the subscription model of direct primary care subscriptions wide open to adverse selection and susceptible to cherry-picking competitions.
In sum, adverse selection is more likely to drive up the costs of paying for primary care through a direct primary care subscription than for primary care through individual market insurance.
In his seminal work, The Economics of Moral Hazard: Comment, Mark Pauly had, according to this account, the “key insight … that full coverage may not be optimal under conditions of moral hazard, that is, when consumer demand for health care responds to the reduced marginal cost of care to the individual.” In Pauly’s own terms, “[When] the cost of the individual’s excess usage is spread over all other purchasers of that insurance, the individual is not prompted to restrain his usage of care…. [Some] medical care expenses will not and should not be insured in an optimal situation.”
Pauly’s attention was directed most pointedly at routine matters like physician visits. Brekke’s scolding, repeated in Parts 1, 2, and 3, that actuarial principles command that patients should simply budget for these “predictable, routine, likely” events rather than buy coverage for them closely echos the Pauly view. Pauly was a genius to figure this out, and Brekke was wise to listen. But she has not applied Pauly’s wisdom across the board.
Pauly’s observation sparked attention to the role of health insurance deductibles as mitigators of moral hazard and seeded the movement toward high deductible health plans (HDHPs). These couple coverage for the “big things” to the use of uninsured cash pay market discipline in regard to shoppable, discretionary services. A high deductible plan is a plausible solution for consumers worried about paying for the excess utilization of primary care services of fellow plan members who succumb to moral hazard.
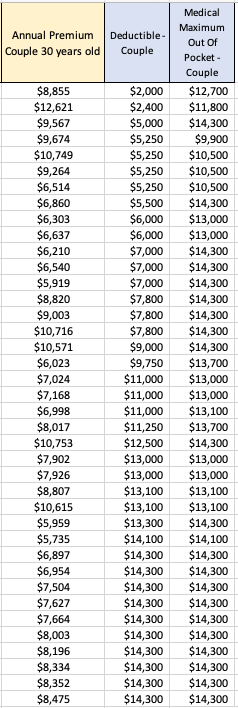
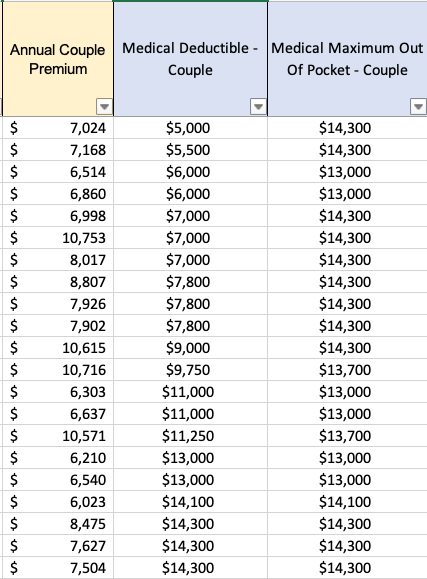
Given that the average deductible in the individual health care insurance market is well north of $3000 for an adult, while typical annual primary care expenditures are less than $1000, moral hazard has largely been mitigated as a contributor to costs — especially costs of primary care — in the individual insurance market.
On the other hand, a consumer who fears paying for excess utilization of primary care services by her fellow plan members had best avoid subscription-based direct primary care plans, which provides unlimited primary care visits at zero marginal cost per visit. Even low deductible insurance policies exert at least some restraint on excess primary care usage, while subscription-based DPC clinics and their most loyal supporters swoon over the complete absence of any such financial restraint. For a recent and typical example, see this blog post — by Gale Brekke! And, it’s part of this very series!
In fact, there is probably no worse primary care scenario from a moral hazard perspective than buffet style, unlimited visit direct primary care. Professor Pauly can be reached at (215) 898-5411; ask him.
Advocacy: DPC gives you unlimited primary care for a regular monthly premium subscription fee. But don’t call it insurance.
Reality: Call it what you whatever you want. Moral hazard will still inflate its costs.
Remarkably, if you peek ahead to Brekke 4, you will see that in her enthusiasm to embrace subscription-based direct primary care, Brekke turned 180 degrees and praised the fact that direct primary care clinics provide subscription-paid coverage for these exact same “uninsurable” primary care events in unlimited number without any per event charge. What was a bug when Brekke 3 applied moral hazard to insurance-based primary care became a feature in Brekke 4 when applied to direct care.
I think Brekke was probably right to the extent she concluded that lower barrier primary care is worth the risk of moral hazard. Still, the moral hazard problem is obviously greatest when the marginal costs of additional visits is zero, as it is in subscription DPC. Brekke was therefore completely wrong in counting moral hazard costs as increasing the relative price of insured primary care over subscription based direct primary care.
To the extent that moral hazard and/or adverse selection are relevant to the choice between paying for primary care with health insurance and paying for primary care directly on a subscription basis, each phenomena would bring higher costs to the direct primary care subscription model. In my responses to Brekke 1 and to Brekke 2, I computed that admin costs of using insurance for primary care could be as high as 15%, shrinking by two-thirds a 50% gap that Brekke had projected. Our review of the issues raised in Brekke 3 makes clear that the cost increases associated with moral hazard and adverse selection can only reduce, and may even reverse, that difference.
We are well on our way to understanding why the $900 annual cost of adult primary care delivered through subscription-based no-insurance direct primary care is more than 50% greater than the $565 annual primary care cost for an adult paying under the insurance system. My response to Brekke 4 will bring us close to home; it should appear at this link when ready.